
When Addiction or Mental Illness Hits Your Family
What We Do
Call Now > 1.310.200.7530 or Toll Free > 1.855.702.7474
“Addiction is a chronic brain disease that has the potential for both recurrence (relapse) and recovery.”
Vivek H. Murthy (MD, MBA), U.S. Surgeon General, 2014–2017, 2021
You can get treatment at a Malibu rehab for $90,000 per month, or for free at 12-step meetings in a church basement . The more resources you have, the more options you have. Conversely, the fewer the resources, the fewer the options. But do more resources alone guarantee recovery? Absolutely not. Whether it’s at a recovery version of Club Med or in a damp basement, recovery is ultimately up to the individual no matter where it occurs.
Treatment is not “one size fits all.”
The key to successful Treatment is matching the Right Treatment with the Right Individual.
That’s where we come in.
What We Do
Intervention
intervention: (1) An unplanned, overwhelming event — overdose, psychotic break, car accident, violence, arrest, incarceration, job loss — that prompts the afflicted to go to treatment. (2) A planned event — crisis intervention by family, friends, colleagues, even oneself — to confront and halt a non-compliant individual’s self-destructive behavior NOW.
Surrender is not guaranteed, but intervention is the final tool the family can use to change their loved one’s behavior. Continued family unity in purpose and action is crucial, or the intervention will fail.
There are two dominant forms of intervention. CRAFT (Community Reinforcement Approach to Family Training) teaches the family to interact non-confrontationally with the individual with positive reinforcement to gradually get the individual to surrender to treatment. However, it can be time-consuming, which risks the family’s patience wearing down and regrettably dangerous if the individual is using substances that can be fatal.
The second form of intervention is remarkably simple because it’s all about LEVERAGE. Something or someone is enabling the victim to continue being addicted, and it has got to come to a screeching halt. You determine the source of the individual’s enablement. A substance-using, 20-something child who is unemployed, living at home, totally dependent upon parents’ support is an all-too-often occurrence. You offer two choices: go immediately to rehab or leave with all enablement from us totally cut off. Now. Other points of leverage include loss of employment, abandonment by family members or incarceration.
1-Year Treatment Plan

The Foundation of successful treatment is a 1-Year Customized Treatment Plan
Understanding each person’s unique physical, psychological, and behavioral needs — plus the intensity and nature of their SUD or mental disorder — leads to outlining a year-long treatment plan that determines the intensity and composition of the first ninety days of formal treatment, followed by an aftercare program. As a person’s lifetime hopefully is a long one, the plan must be continually assessed and modified to meet the individual’s changing needs.
Our Top 10 Specs
In considering the right rehab for clients, here are our Top 10 specifications that must be met:
1 Diagnosis
To get the right treatment, it’s necessary to know what needs to be treated. That’s when we need a diagnosis based on a clinical assessment by a certified, licensed behavioral health professional either in person, via video or over-the-phone.
Since addiction is a disease of the brain, it frequently occurs with other mental disorders. The question is which disorder is driving the other? Does the mental disorder(s) drive the substance use or does the substance use drive or induce the mental disorder? Either way, today’s research indicates that both illnesses should be treated in an integrated fashion.
A professional diagnosis reveals one of the following:
Single Malady
Substance use disorder (SUD)
Mental Health (MH)
Co-Occurring Maladies
Primary SUD + Secondary MH
Primary MH + Secondary SUD
2 Licensure
Treatment is not a one-size fits all solution to a complex, life-long endeavor. It has to start with one’s diagnosis matching the licensure of the treatment program. Treatment facilities need to be licensed by the state in which they practice, therefore, knowing a facility’s licensure is key when determining the ones to be considered. Licensure normally falls into one of the four categories listed above, plus some programs have two primary licensures: Primary MH AND Primary SUD.
Licensure
Primary Only
Substance use disorder (SUD)
Mental Health (MH)
Co-Occurring
Primary SUD + Secondary MH
Primary MH + Secondary SUD
Dual Primary
Primary SUD
&
Primary MH
3 Disorders Treated
Substance Use Disorder (SUD) is a chronic brain disease causing the inability to control the impulse to use a substance or stop repeating a process despite devastating consequences. As a chronic disease, it alters a person’s brain structure and function. It is not the result of a moral failing, bad character, or lack of willpower, though some unenlightened people still believe that.
Rehabs treat Substance Addictions that are primarily grouped into four major categories:
Alcohol
Beer
Wine
Malt Liquor
Distilled Spirits
Illicit Drugs
Cocaine, including Crack
Heroin
Hallucinogens: LSD, PCP, Ecstasy,
Peyote, Mescaline, Psilocybin
Opium
Methamphetamines, including Crystal Meth
Marijuana, including Hashish
Synthetic Drugs: K2, Spice, Bath Salts
Household and Industrial Substances (Inhalants)
Amyl Nitrate
Cleaning Fluids
Gasoline
Lighter Gasses
Anesthetics
Solvents
Spray Paint
Nitrous Oxide
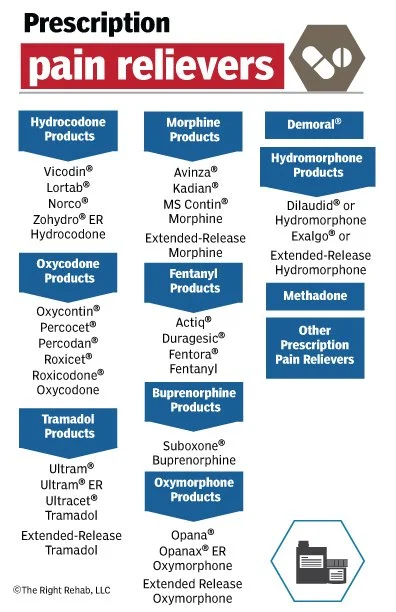
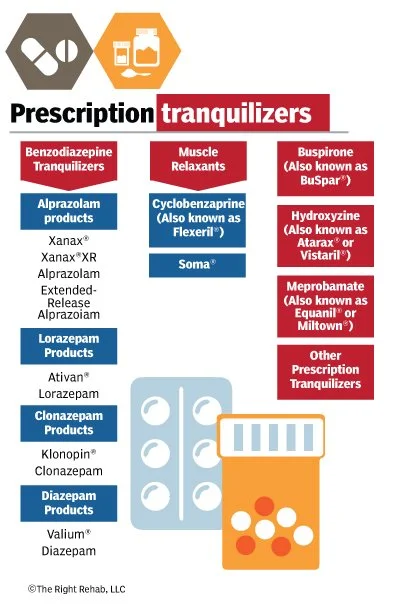
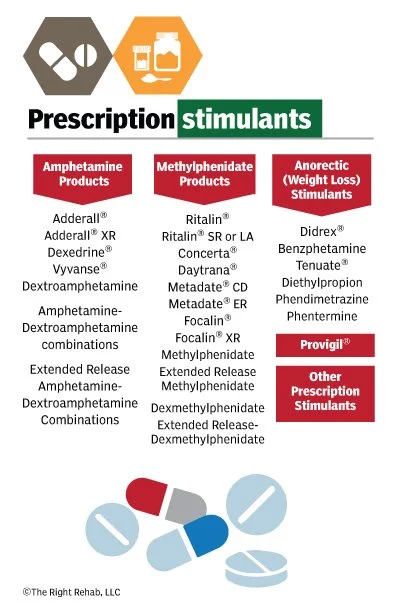
Legal Drugs Used Illicitly
Pain Relievers
Tranquilizers
Stimulants
Sedatives

Mental Disorder: An adult having any mental, behavioral, or emotional disorder in the past year that ranges from none to mild impairment for two weeks or less, all the way up to full-blown schizophrenia, has an AMI (Any Mental Illness). Adults with AMI are defined as having SMI (Serious Mental Illness) if they have any mental, behavioral, or emotional disorder that substantially interferes with or limits one or more major life activities. Symptoms of SMI include the inability to work, function in school, interact with family, and fulfill other major life activities. AMI and SMI are not mutually exclusive.
“Mental Illness,” National Institute of Mental Health, https://www.nimh.nih.gov/health/statistics/mental-illness.shtml
Common Mental Disorders
Depression
Anxiety/Panic Attacks
Schizophrenia
Trauma - PTSD
Personality Disorder
Bipolar Disorder
Obsessive/Compulsive Disorder
Impulse Control
Anger Issues
ADHD
Bulimia
Process Addiction: Considered a mental disorder, not SUD, it is obsessive behavior not necessarily accompanied by substance use that compels the individual to engage compulsively and repeatedly in conduct detrimental to the individual.
Process Addiction
Eating Disorder
Gambling
Sex & Intimacy
Love
Pornography
Work
Compulsive Buying/Shopping
Internet
Self-Harming
Codependency
Gaming
4 Levels of Treatment / ALS

A key factor when evaluating a rehab is their patients’ Average Length of Stay (ALS). Is the program a stand-alone 30-day residential program? Do they have their own Partial Hospitalization Programming (PHP) and Intensive Outpatient Programming (IOP) or do they refer patients to other ones? The ALS could also be a long-term program way past 90-days — 6 x months, 9 or 12 x months or longer.
5 Demographics & Setting
Where do our clients fit within the demographics of the facility’s population?
What is the facility’s capacity and current population? Gender ratio?
Which age groups does it treat?
Pre-teen 5–12
Adolescents 12–18
Youth 18–26
Adults 26 – above
Seniors 65+
Gender: Male, Female, LGBTQ, Non-Binary, Trans?
Are there gender-specific group sessions and living quarters?
Are there specific therapeutic tracks or stand-alone programs for professionals?
Attorneys
Physicians/Nurses
Pilots
Business Executives
Active Military/Veterans
1st Responders (Police, Fire, Rescue)
Faith-based
What is the size of the campus?
What is the setting?
Urban?
Rural?
Suburban?
Residential neighborhood?
6 Treatment Team & Therapies
Who are the Team members working with my client?
Levels of degrees (PhD, Masters, PA)
Psychiatrist
Principle therapist
Trauma Therapist
Family Therapist
Equine Therapist
Case Manager
Discharge Planner
Nurse
What is the daily and weekly treatment regimen
Number of individual sessions per week?
Additional individual sessions available?
Number of group sessions per day/week?
Number of family, trauma, equine sessions per week?
Which Evidence-based therapies and modalities are practiced?
CBT (cognitive behavioral therapy)
DBT (dialectical behavioral therapy)
FBT (family behavioral therapy)
BCT (behavioral couples therapy)
EMDR (eye movement desensitization and reprocessing)
Brainspotting
Psychodrama
Relapse prevention
Equine therapy
MAT (Medication-assisted therapy)
12-step meetings (on- and off-campus)
Hypnotherapy
Psycho-ed
LifeSkills
Earn GED
7 Location
A totally new environment offers a critical component in the individual’s treatment — an opportunity to leave the previous life of addiction and addiction-related relationships physically behind.
Placing the patient into a treatment facility at or near one’s home cannot be a priority. I often hear, “we would like him to be close to home so we can see him at any time or if there’s a problem.” NO. The problem is him being too close to the world from which he needs to escape. That includes family. We must also eliminate an easy exit out the door or have a friend come by to pick him up.
I tell parents of a Gen Z offspring, “the phone call you want is, ‘I’m not coming home.’” What that means is that he’s found a new life, one of sobriety, positive mental health and recovery. His friends and relationships—his whole environment — is no longer centered on drugs and their destructive habits. Now he has the support to build a new, sober life. One rule for those other than adolescents and adults with family /employment obligations or for criminal justice issues: one should not return home for at least one year, and that’s only for a brief visit.
8 Accreditation
Two out of these three or all three of these accreditations are essential to be considered as the Right Rehab for the Right Person.
The National Association of Addiction Treatment Professionals (NAATP) is the ultimate umpire in the $142 billion per year (and growing) treatment industry. If a facility violates NAATP’s code of ethics, they’re called out and possibly expelled.


Certification by one or both CARF International (the Commission on Accreditation of Rehabilitation Facilities) or the Joint Commission. Both are nonprofit accreditors of health care service providers. Beware of rehabs that fraudulently display one or more of these seals. If I see a facility’s website displaying a seal I believe could be fraudulent, it often is and I call it in to the association.
9 Insurance: In and Out-of-Network Status
Regardless of one’s economic status, clients who have health insurance most often use it to the fullest extent of its usefulness.
Deductible is the amount the individual pays for covered services or medications before their insurance starts to pay. Out-of-pocket-maximum is the predetermined amount of money that an individual must pay before an insurance company pays 100% of covered expenses. After the deductible is met, that amount folds into the out-of-pocket limit. The insured is then responsible for a co-pay schedule on covered services until the Out-of-pocket-maximum is met, thereafter, the insurance company pays 100% of clinical services.
The in or out-of-network status of your insurance is dealt with the following ways:
In-network:
The rehab and client’s insurance carrier have a previously agreed upon schedule of reimbursement rates for all levels of treatment.
The client pays upfront the unmet portion of the individual’s out-of-pocket maximum (OOPM) to the rehab prior to start of treatment. Thereafter, the insurance company will pick up 100% of clinical care it authorizes and sends those payments directly to the rehab during treatment.
After the residential treatment stage, the client is stepped down to PHP and then IOP, thereupon the client is responsible for subsequent housing and ancillary fees. Insurance covers only the clinical portion of treatment.
Out-of-network (1)
There is no in-network-type reimbursement agreement between the rehab and insurance company, however, it is common for them to arrange a “single case agreement (SCA).”
The client pays the unmet portion of the OOPM directly upfront to the rehab. (The OOPM at an out-of-network facility is most often twice the amount at an In-Network facility.)
The insurance company sends the agreed upon reimbursement fees directly to the rehab during treatment.
If the insurance company’s fees are considered adequate by the facility for its clinical services, the Client thereafter is only responsible for subsequent housing and ancillary fees upon being stepped-down from residential to outpatient treatment.
Out-of-network (2):
The client pays cash upfront for all treatment and clinical services prior to commencement of treatment.
As a courtesy, the facility files with the client’s carrier for out-of-network benefits during treatment.
Any benefits are paid directly to the client.
Out-of-network (3):
The client pays cash upfront for all treatment and services.
As a courtesy, the facility files with the carrier for out-of-network benefits after treatment.
Any benefits paid by the insurance company go directly to the client.
Out-of-network (4):
The client pays cash upfront for all treatment and services.
After treatment, the facility gives the client a “superbill” of all charges paid by the client.
The facility introduces the client to a 3rd party company specialized in getting out-of-network benefits (for a fee) from the insurance company to the client.
Out-of-network (5):
The client pays cash upfront for all treatment and services.
After treatment, the facility gives the client a “superbill” of all charges paid by the client.
Filing for out-of-network benefits is the client’s responsibility.
10 Paying for Treatment
Which payment platforms do they accept?
The costs of treatment are mostly covered by a combination of several sources such as private health insurance + private pay; Medicaid + other public assistance; or cash for residential treatment + insurance that only covers outpatient programming.
Public Assistance

Treatment funded by one or more federal, state, local programs including State mental health agency funds, adult & juvenile courts, welfare & family services, tribal funds, private or community foundations, etc. that are available in one’s state of residence.
Scholarship

Most rehabs set aside a budget for giving scholarships to those in need of treatment but without the resources. Since each facility has its own particular program and timing, you cannot rely on one being available when needed.
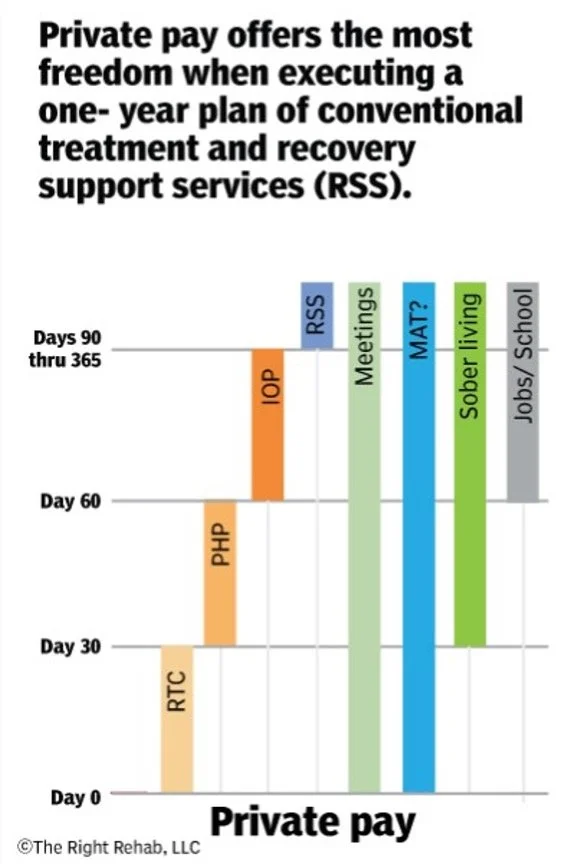
Cash / Private Pay
The key advantage of paying with cash ($15,000-to-$100,000 per month) is the actual receipt of 90-days or more of treatment that the facility controls without needing an insurance company’s authorization.
Government Sponsored Insurance

Tricare
The most common health insurance for over 9.9 million active military, their families, reservists and retirees. Fortunately, Tricare is increasingly available in rehabs across the nation, especially at upscale ones that are normally financially out-of-reach for most in need. CHAMP/US and CHAMP/VA are other programs for veterans and their family members.
Medicare
Covers 61 million seniors who are 65 and over, plus over 6 million of those disabled and under 65. Although Medicare inpatient coverage for stabilization is ubiquitous in hospitals throughout the nation, its coverage of a 30-day residential stay for addiction and/or mental health is practically non-existent. It is, however, often liberal in the number of days it covers for outpatient addiction and/or mental health treatment, although it does not cover the costs of housing, if needed, during that care.
Medicaid and CHIP
Covering 79.6 million, Medicaid is a federal / state partnership providing health care coverage for low-income Americans between the ages of nineteen and sixty-four years old. Covering in excess of 20 percent (or one in five) of Americans, it’s also responsible for 20 percent of all health care spending in the United States, including major funding for hospitals, community health centers, and nursing homes. CHIP is the Children’s Health Insurance Program (CHIP) covering 7.1 million low-income children, pregnant women, adults, seniors, and people with disabilities. A primary goal of the program is to protect individuals and families from financial strain.
Private Group and Nongroup Insurance

Getting ninety days of formal treatment starting with residential solely through one’s employer-sponsored or nongroup insurance is a pipedream. However, if you have access to supplemental cash, your policy can dramatically contribute to treatment at a facility that otherwise would be unaffordable. It’s my job to make that happen.
Employer-sponsored health insurance covers the largest group of individuals and families at 167.3 million. An additional 17.4 million get their coverage through Marketplce.gov and 21.3 million have nongroup insurance via independent agents.